A 2020 guest series by Anne Maloney, inspired by James Taranto.
A Bye-Ku for Seth Moulton
Strove for the center
But Dems want only left turns
Back to Salem, Seth.

A 2020 guest series by Anne Maloney, inspired by James Taranto.
A Bye-Ku for Seth Moulton
Strove for the center
But Dems want only left turns
Back to Salem, Seth.
 A 2020 guest series by Anne Maloney, inspired by James Taranto.
A 2020 guest series by Anne Maloney, inspired by James Taranto.
A Bye-Ku for Jay Inslee
Back to Seattle
chilly climate never warmed
to Pres. Jay Inslee.
Trump’s current approval rating is pretty similar to the approval rating for both Obama and Reagan at this point in their respective presidencies. (Trump 43%, Obama 45%, Reagan 43%.)
Reagan’s recovered sharply over the course of the election year, and he was comfortably over 50% when he faced Mondale.
Obama didn’t really recover, but he managed to pump his approval rating up to about 47% during much of the campaign, and squeezed it up to 49% during the last days of his re-election campaign, which got him narrowly re-elected.
(Obama’s approval promptly slumped again after his second inauguration, and he remained pretty unpopular until his lame-duck period suddenly made him the most popular politician in America.)
Most presidents see modest gains in their approval ratings during an election, probably because (partly) they’re no longer being compared to a non-existent ideal but to the actual flawed human opponent and (partly) all that presidential campaign advertising pays off marginally.
George H.W. Bush and Jimmy Carter are the big exceptions. H.W. was hit by an election year recession for which he was (rather unfairly) blamed. Carter never recovered from the failure of Operation Eagle Claw, the military attempt to rescue the Iranian hostages, and his subsequent address to the nation.
That recession in the Bush I Administration is something Trump should watch out for.
Another thing Trump should watch out for: both Obama and Reagan started their presidencies well above 50%, proving it was theoretically possible for them to win majority approval. President Trump’s best approval rating came on his very first day in office… when it was only 45%. Trump may have a much harder time reaching 49% than Obama or Reagan, because that would be all-new territory for him.
A 2020 guest series by Anne Maloney, inspired by James Taranto.
A Bye-Ku for John Hickenlooper
A Hickenlooper
Cannot be the President
His name’s too funny.
A 2020 guest series by Anne Maloney, inspired by James Taranto.
A Bye-Ku for Eric Swalwell
Back to Golden State
With your viral Eric hair
Not bold, big or good.

“Error has no rights.”
It’s not clear where this axiom comes from. (Some say the Inquisition. I can’t find it before Orestes Brownson, who critiqued it.)
Yet the axiom seems correct to me, and I think, at some level, most people believe it. If a child tries to walk into traffic, you don’t say, “Oh, well, that’s interesting, I don’t agree with it but I defend your right to try it.” No: you grab the child! He has erred and he needs to be corrected! And when a grown man says, “I’d like to kill your family,” the natural, normal human response is not to “answer his speech with more speech.” It’s to try to arrest, disable, or kill the man before he has a chance to do anything to your family!
Which, naturally, brings us to Nazis.
There are people in our country today who want to kill all the Jews. Or all the non-Whites. Or both. They can be found marching in the streets in some places. When they post about it online, they pretend to be “just kidding,” but you must not believe them:
The unindoctrinated should not be able to tell if we are joking or not. There should also be a conscious awareness of mocking stereotypes of hateful racists. I usually think of this as self deprecating humor – I am a racist making fun of stereotype of racists, because I don’t take myself super-seriously. This is obviously a ploy and I actually do want to gas kikes. But that’s neither here nor there.
-Andrew Anglin, Daily Stormer style guide
This evil minority “actually does want to gas kikes.” They advocate a totalitarian state that suppresses any ideas contrary to their particular vision of their deranged “Aryan” racial ideology. Nazis have erred in an extremely dangerous way. It is imperative that they be prevented from enacting any of their horrifying agenda. And even allowing them to spread their ideas, even to privately hold these ideas, is dangerous. Why should any society protect this? Why should any Christian or humanist suffer such people to preach their hatred?
So punch ’em! That’s what a lot of people are saying these days: get violent! Attack neo-Nazis with force! You’ve probably read about the assault on prominent white nationalist Richard Spencer. You may not have seen the left-wing “blue checkmark” class openly celebrating the attack (here’s a major Obama speechwriter, for instance). You may not have seen one of America’s big-three television networks explicitly endorsing anti-Nazi violence in a direct-to-audience monologue on The Good Fight:
Is it alright to hit a Nazi unprovoked? I was always taught never to throw the first punch, never to instigate. Defend, but don’t attack. But then I saw a video of the white nationalist Richard Spencer being punched in the face during an interview. I realized Spencer was in a pressed suit, wearing a tie, being interviewed like his opinion mattered — like it should be considered part of the conversation, like neo-Nazism is just one political point of view. And then I realized there’s no better way to show some speech is not equal. Some speech requires a more visceral response. It’s like Overton’s window — that’s the term for which ideas are tolerated in public discourse. Well, Overton’s window doesn’t mean shit unless it comes with some enforcement. So yeah, this is enforcement. It’s time to punch a few Nazis.
A significant American television program, with a sizable budget, hundreds of staffers, and an estimated several hundred thousand viewers, came out and told Americans they should punch Nazis.
And, y’know, there’s something to this!
The Nazis themselves endorse terrible violence against vast numbers of people for truly absurd reasons, and they want to destroy the free-speech protections for everybody who dissents from their tyrannical aims. The threat their continued existence poses is not trivial. The last time around, Nazis took power through the ordinary political process, then promptly killed 12 million of their own people (not to mention the 50 million who died in the war they launched) and policed the rest of the population with a horrific secret-police state.
But they complain when the rest of us consider stripping their free-speech rights and performing some (relatively modest) violence against them?
If ever there was an error that earned harsh, coercive correction–even violent correction–Nazism is it.
Yet I think it is a very bad idea to go around punching Nazis. The growing support for anti-Nazi violence is cause for alarm.
Yes, I agree that, by nature, error has no rights.
But we have chosen, as a society, to give error some rights.
Consider the First Amendment. It grants all Americans a freedom of speech. Why? It’s not there to ensure citizens have the right to agree with the government and the majority. The government and the majority can already express themselves without fear of punishment, because they are the government and the majority! So the First Amendment is there to protect the speech of dissidents. Speech that opposes the government and the majority. Speech that the people in power consider erroneous.
The First Amendment also furnishes you a right to exercise your religion. Is that there to protect the popular State religion? No! It’s there to ensure that citizens are free to practice false religions. In England and Colonial America, religions like Quakerism and my own Catholicism were officially considered false and therefore gravely dangerous. They, not the Anglicans, are the real beneficiaries of the Free Exercise Clause.
The First Amendment also guarantees that you can petition the government for redress of stupid grievances, and to publish dangerous ideas and facts in the press.
We’ve given error rights. Heck, we’ve made “error has rights” the very center of system of government! We call this reverence for error “liberalism,” and it is bizarre, unnatural, and profoundly counterintuitive.
It has also been stupidly successful.
Liberalism has benefited our society in many ways, too numerous to list here. Our science, our literature, our art, our economy, our political stability, are all buttressed by liberalism, allowing our material standard of living to fly to heights undreamed of in human history. I wish to focus on just one aspect of liberalism here: the way liberalism has helped restrain ideological violence.
Throughout human history, people have slaughtered each other, even their own neighbors, by the thousands and the millions, because they believed different things. Catholics slaughtered the Cathars because they feared Cathar ideas could spread and imperil the salvation of the faithful–damnation being a fate even worse than death. Anglicans slaughtered Catholics for more or less the same reason. Communists slaughtered kulaks (and still slaughter Uyghurs): same reason. French Revolutionaries slaughtered just about everyone, including their own revolutionary heroes, for the slightest past deviation from the current party line. Even the tolerant Romans feared that people who refused to participate in pagan civic sacrifices would call down the wrath of the gods… and so they slaughtered such “atheists.” The river of history runs red with the blood of dissenters.
But not here. Not now. We don’t kill our dissenters.
Indeed, we often listen to them, because, from time to time, there’s a grain of truth in what our dissenters are saying–one we need to hear. Sometimes, our dissenters turn out to be altogether correct. Where would we be if we’d enforced our beliefs and muzzled theirs? Well, have you seen HBO’s Chernobyl? Do you remember the Mortara Affair? Have you checked out China’s new social credit system? A political system closed to radical critique does not end up good for anybody.
Even when our dissidents are completely wrong, sanctioning them would only make them stronger, thanks to the Streisand Effect. You can spend a trillion dollars on Chinese-style censorship or you can spend zero dollars and let somebody else write an effective rebuttal. This single post almost single-handedly removed Michael Anissimov and his brand of neoreaction from circulation. (He has now deleted his website and even removed its archive from the Wayback Machine, proving he was always a monster.) Counterspeech may not be natural, but it works.
Forcing bad ideas into a closet of suppressed speech, on the other hand, lends them the credibility of samizdat and makes establishment channels look like Pravda; thus, dangerous ideas are not defeated, but fester and grow. If openness means we have to put up with birthers and alternative medicine loons on Twitter? Seems like a worthwhile price to pay.
My mother, who is a college professor, told me the story of an exchange student from Liberia during the 2000 election. It’s a liberal college campus, so, naturally, after the wild events in Florida on election night (read up, kids), most everyone came to class to depressed. It was still not clear who would be elected President; I myself, at the age of 11, found the whole thing thrilling, remained glued to the screen for five weeks, and that was when I started really paying attention to politics.
But the Liberian student seemed neither glum nor excited. She seemed nervous. After class, she asked my mother when the military would be putting tanks in the streets to keep the peace. My mother, of course, was shocked by the question. The electoral college is idiosyncratic (and very good), Florida’s ballots were a mess, and there was a lot riding on the election outcome… but she knew Al Gore would have his day in court and the matter would be settled peacefully, for good or ill. My mom’s student, on the other hand, had spent her entire life in a country seized by coups, warlords, and civil war. The idea of a contentious but fair election culminating in a peaceful transfer of power to the loyal opposition was just as shocking to her.
We have an exhausting, ugly, deeply flawed Discourse in this country, full of demagoguery and online mobs and confirmation bias and outrage and plain old lies. Liberalism itself contains serious theoretical defects and practical consequences. And yet, for all that… people do not kill each other over ideas in this country. At the end of the day, that’s what liberalism has bought us. Giving error rights has given us the breathing room we need to live in peace and forge a nation E Pluribus Unum. This personal safety is so much a fixture of our national mindset that we easily forget how extraordinary it is–and how fragile.
But what does any of this have to do with Nazis? Everybody agrees Nazis are bad. Everybody agrees they don’t really deserve a right to their error. Can’t we make an exception for them? Instead of absolute liberalism, where we say, “People have a right to their errors,” couldn’t we change it to, “People have a right to their errors, except Nazis”? Then we could finally fix the Nazi problem for good, without hurting anybody else! Anyone can see the appeal.
But I promised two reasons not to punch Nazis, and here’s the first: who decides what counts as a Nazi?
It’s easy enough to say, “Yes, let’s all go punch Andrew Anglin.” He’s an avowed Nazi who, as we’ve noted, avowedly “wants to gas kikes.” Definitely a Nazi. Oughta get punched.
It’s also not too hard to want to punch Richard Spencer. Spencer personally denies that he’s a Nazi, but that’s pretty hard to believe when you read the things he says, particularly his regular, subtle, favorable invocations of Nazism. He’s totally a Nazi, just lying about it. Go punch him, too, right?
But, just this week, no less an entity than The New Yorker, the definitive American journal of letters, made an extended case that President Donald Trump is a Nazi. Uh-oh.
Trump says he isn’t a Nazi. But so does Spencer, and Spencer’s definitely a Nazi, so Trump’s denial doesn’t settle anything. We must turn to the evidence.
Does Trump want to kill all the Jews? If he does, moving the U.S. Embassy to Jerusalem was a pretty odd way of showing it. But does he want to kill a lot of Central Americans? Well… that’s under pretty intense dispute right now: there’s no question that Central American asylum-seekers are dying at ridiculous rates because of outrageous lapses in logistics and supplies. Is this because the border is overwhelmed by asylum seekers, or because President Trump wants them to suffer, even die? (Both?) If the latter, does that make him a Nazi?
I know plenty of people who say, “Yes, Trump is the same as Hitler,” without a moment’s hesitation. Now, I think that’s a pretty crazy comparison, but that’s just me. I can’t stop other people from concluding — even erroneously — that Trump = Hitler. Trust me, I’ve tried!
So now our narrow little exception to liberalism, our small allowance for errors that are so serious we should silence them with the threat of violence, has suddenly widened from “a handful of dudes on fringe Internet sites who want to gas Jews” to “fringe internet trolls… plus the current President of the United States and much of his administration.”
But we can’t stop there. We also have to deal with Trump’s supporters. If Trump is a Nazi, doesn’t that imply that his supporters are also Nazis, rank-and-file brownshirts complicit in his evil acts? Seems to follow logically. This guy on MSNBC sure thinks it does. A very dear friend of mine recently wrote on Facebook about the immigration detention camps under President Trump and noted, in conclusion, “If you… support it, you are my enemy, and I would lift a weapon against you in violence if it would do a single thing to help those people.” That presumably includes all of the 43% of the American public that currently approves of President Trump’s job performance.
It’s not just Trump, either. I’m not a Trump supporter, but I was a George W. Bush supporter, and I’m old enough to remember when Bush and all his supporters were quite routinely compared with Hitler and the brownshirts. I remember watching, of all things, a Star Trek fan film that opened with a list of great Earth dictators condemned by history: Hitler, Stalin, and George W. Bush. Labeling Republican presidents Nazis has been a hobby since Barry Goldwater ran for President, so I’m pretty sure there’s nothing special about Trump. If Marco Rubio were President, the same people would be calling him and his supporters Nazis. They always have, so why stop now?
If we all agree that it’s okay to perpetrate violence against Nazis, and if a fair number of us believe that everybody who votes for any Republican for President is a Nazi…
…uh-oh.
We poked one hole — one tiny tiny little hole — in the fabric of liberalism. All we wanted to do was make one little exception to the “right to be wrong” we’ve invented for our society. We wanted to give ourselves the ability to be intolerant of the most extreme intolerance.
Before we can even blink, we find that a big swath of us have found a way to use this to justify intolerance and violence, not toward some tiny extremist minority nobody will miss, but toward something like half the United States population! That’s not a slippery slope: it directly follows from the belief that it’s okay to punch Nazis and the surprisingly common belief that Republicans are morally equivalent to Nazis. Our “one hole” has blown half the dike!
And we’re not even done!
So far, we’ve only talked about how left-wing people might use liberalism’s hypothetical “Nazi exception” in order to legitimize ideological violence against vast swaths of the population. But, once we’ve drilled a hole in liberalism to make punching evildoers okay, do you really think the Left is the only side that’s going to start throwing as many ideological enemies into that pigeonhole as they can?
Heck no! The Right has spent generations resenting how Nazis are considered The Worst People In History but Communists (especially Stalinists) are tolerated with a wink and a nod, considered serious subjects for sympathetic academic study, and even considered a bit cool. All this despite the fact (and this is true) that Communists very likely caused more deaths with just as much grotesque horror as anything conjured in the feral pits of Adolf Hitler’s mind. John Zmirak wrote a very amusing satire of this double standard about a decade ago in Taki’s, a vile magazine that is a victim of this very double standard. If we’ve decided Nazis are so bad that they need to be fought, then surely the same goes for Communists.
Which leads to the Right starting purges of university faculties and scientific associations, getting rid of their communists and their communist sympathizers — and maybe burning a few books while they’re in the neighborhood. The Right will feel completely justified about doing this, because, after all, Communism is an extremely serious and dangerous error that kills millions of people! Such serious errors have no rights! “We can’t tolerate the intolerant!” the Breitbart columnists will agree as they toss another copy of Das Capital on the flames.
One more and I’ll let you go.
The really awful thing about Nazis is that they killed millions of innocent people in industrialized death centers, right? There’ve been plenty of unfree governments in history, but “callously butchering 12 million men, women, and children” is the thing that makes the Nazis the worst people in history, right? Even their ideas are so dangerous that we’re talking about suppressing them even before they actually do anything horrible.
Well, hi! I’m pro-life, and would you care to guess how many babies Planned Parenthood has killed? Actually killed, not just talked about it? It’s a good many more than 12 million. If it’s okay to punch Andrew Anglin because he wants to kill Jews, than Scott Roeder, who put a stop to George Tiller’s prolific career of child-murder, is a big damn hero. If anti-Nazi violence is okay because the Nazis might theoretically someday start killing racial minorities, then surely the violent destruction of every active abortion mill in America is a downright moral imperative! Right?
You think that’s a silly comparison? Well, I thought the whole “Trump is like Hitler” thing was pretty silly. But, as with the Trump is Hitler thing, millions and millions of Americans believe Planned Parenthood is Dachau. I myself am so serious about this precisely because I spent years considering the morality of anti-abortion ideological violence, and I have seen where that logic leads. Once ideological violence is normalized, what makes you think you can stop it from targeting PP?
Starting to feel a little shaky about the whole “punching Nazis” enterprise?
You should! We’ve now blown the entire dam. We began with liberalism, which says that people have a right to be wrong, even about important things, and that “error has rights.” We like liberalism because it’s given us an incredibly free and peaceful society, where ideological violence is essentially unheard of. We then tried to make an exception allowing us to enact ideological violence against one tiny and universally hated group, one which would do the same to us given half a chance. What could go wrong?
But it turns out that the boundaries of that “one tiny and universally hated group” are by no means universally agreed upon. Which means that our “one little exception” to liberalism isn’t so little after all. We end up justifying ideological violence by… pretty much anyone… against… well, pretty much everyone. In other words, we’ve blown up liberalism. Our exception has swallowed the rule. Error is once again deprived of any rights, and we’re back to killing each other like Catholics and Cathars. Of course, our culture no longer cares enough about religion to bother policing merely religious heresies; the heretics we persecute have erred about far more important things, like Halloween costumes.
It does no good to say, “Well, we’ll just have the government decide which hate speech counts as Nazi enough to be suppressed.” When the government sets up hate-speech tribunals, it inevitably does the same thing the rest of us do: it massively broadens the definition of “Nazi” to serve their interests and deplatform their enemies. In a right-wing government, you get the House Committee on Un-American Activities. In a left-wing government, it’s the Colorado Civil Rights Commission. Either way, the only thing you’ve done is taken all the problems described above and added an Inquisition on top.
So that’s the first reason why we should not punch Nazis. Once you stop tolerating intolerance, society’s definition of “intolerance” rapidly broadens. We stop tolerating disagreement on any sufficiently important issue. We characterize such disagreement as “violence,” and then we respond to that “violence” with actual violence. Pretty much everybody loses. You lose, I lose, the Right loses, the Left loses, the stability of our whole society loses. You know who doesn’t lose?
The Nazis, that’s who. The Nazis want nothing more than for us to start punching them. Which brings us to Reason Number Two not to punch Nazis.
Adolf Hitler’s rise to power is a very complicated historical event. There are a lot of different narratives you can use to explain it, and most of them are true. Getting at the complete big picture takes a lot of work. But here is one true telling of the Nazi rise to power in Weimar Germany:
After World War I and the abdication of the Kaiser, a new, republican system of government formed in Germany. However, left-wing communist radicals, backed by the Soviet Union, opposed this government and violently revolted against it, attempting to impose a totalitarian Bolshevik state. After the failure of the January Revolt of 1919, left-wing paramilitary outfits continue to engage in campaigns of street violence and terror against their political opponents. The Weimar government was, on its own, too weak to suppress the communist violence. Instead, military veterans formed what were essentially street gangs called Freikorps, which answered left-wing street violence with right-wing street violence. As the violence continued to spiral throughout the 1920s, complete with a coup or two, the credibility of the moderate centrist party (the SPD) suffered. Their monopoly on violence collapsed completely. Both the communists and the anti-communists became more polarized… and more organized.
Ordinary, middle-class voters were scared of the communists, who could and did take harsh action against their “class enemies,” including the middle-class bourgeoisie. Ordinary, middle-class voters could not count on protection from the weak central government. Indeed, the head of the German communists, a violent revolutionary and honest-to-God Stalinist named Ernst Thälmann, enjoyed enough support to be considered a credible candidate for German leadership — even as Thälmann ordered his paramilitary, the “antifa” Red Front, to wage war against mainstream right-wingers and centrists for being “social fascists.” (I wasn’t joking when I said above that intolerance for fascism quickly turns into intolerance for all political opposition. This is but one example from a century full of examples.)
However, middle-class voters were not without hope. Through their organization, their numbers, and their record of accomplishments, middle-class voters knew that they could count on another force to protect them from the Communists: the Sturmabteilung, one of several spiritual successors to the disbanded Freikorps. This anti-communist organization commanded some 60,000 men, including a motorized division for rapid mustering. They had been very effective at defending right-wing speakers against communist violence, and they had inflicted quite a bit of retaliatory violence against left-wing speakers as well. And so, in large part hoping simply to protect themselves and their neighbors from the unhinged “antifa” left, enough scared German voters went to the polls in 1930 to make the SA’s leader the second-most powerful man in Germany.
That leader was Adolf Hitler. The SA was the paramilitary arm of his Nazi Party.
(The communists finished third. It is interesting to speculate whether history would have turned out better or worse had Thälmann ultimately taken power instead of Hitler.)
The Nazis came to power, then, not because liberalism was too tolerant and refused to punch Nazis. The Nazis came to power because liberalism broke down. The Nazis came to power because people started punching Nazis (and, soon enough, everybody else in the political right or center), and, as liberalism collapsed, the Nazis were the only ones who could plausibly promise to restore order and protect ordinary voters from the consequences.
Karl Popper was wrong. (And his latter-day exponents are much wronger.) Under liberalism, tolerance of other ideologies must be absolute. If their proponents commit crimes, go ahead and bring them in through ordinary due process, but the “crime” needs to be more than “this guy believes an evil ideology.” If you try to carve out exceptions where we don’t have to tolerate violent or intolerant ideologies, then liberalism destroys itself, the violent come to power, and you end up in the same place as nearly every other society in history before we invented liberalism: living under authoritarianism.
So, one reason to punch Nazis: they deserve it.
Two reasons not to: everyone ends up getting punched, and the ensuing violence only makes the Nazis stronger.
Don’t punch Nazis.
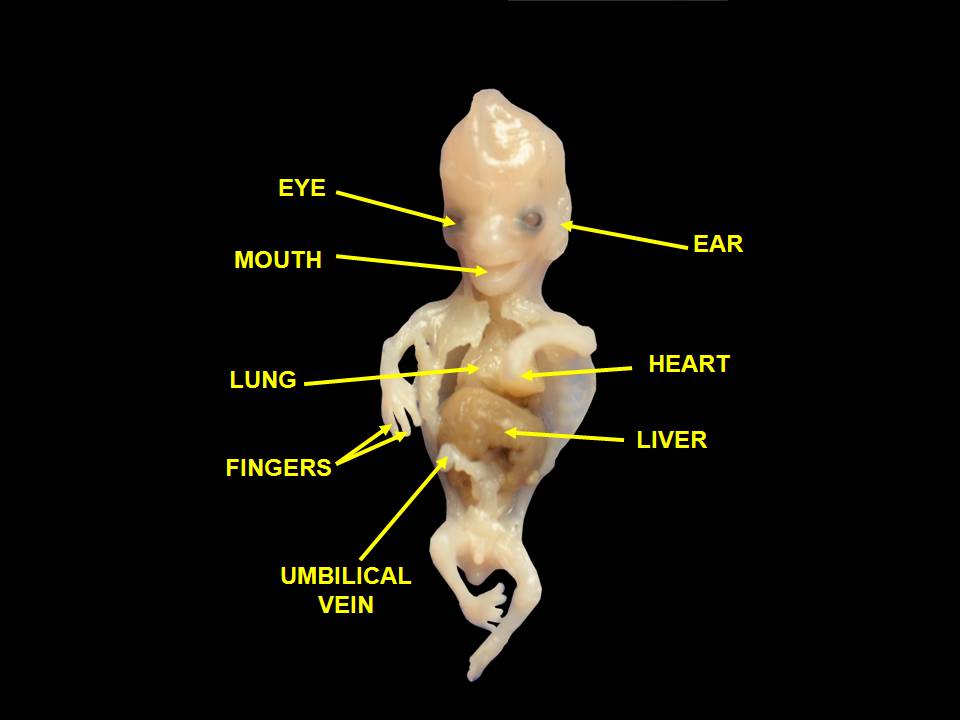
![[extremely Doc Brown voice] EIGHTY EIGHT BEATS PER MINUTE!**](https://www.jamesjheaney.com/wp-content/uploads/2019/07/2037_Embryonic_Development_of_Heart.jpg)
This strategy is somewhat successful, because many voters are comfortable with legal abortion on demand as long as the child is still a “blob of cells,” but become uncomfortable once the child begins to take on human characteristics like a heartbeat. No one would accuse this view of coherence, but that’s life in a country with a vast, muddled middle on abortion. You attach unborn-child protections to a relatable human milestone, and you can gin up the votes to get them passed in a few states.
Of course, the pro-choice Cathedral* is unhappy about this. If there is a conflict between the political underpinnings of abortion rights and reality, it is always reality that has to go. (We’ve seen this before on this blog… and, of course, the very term “pro-choice” is a euphemism: what choice? Who, whom?)
So, on May 31st, the press dutifully invented a brand new term for fetal heartbeat: “embryonic pulsing.” A few days after that, the American College of Obstetricians and Gynecologists (ACOG) announced the henceforth official terminology for “fetal heartbeat”: “electrically induced flickering of a portion of the fetal tissue that will become the heart.”
This whole thing was a bit awkward. Ordinarily, the journalism arm of the Cathedral knows better than to start using the new euphemisms before they have been officially promulgated by the “medical experts.” The New York Times jumped the gun, which exposed the game they are playing.
We should take a moment to notice that, despite ACOG’s official decree, it’s not actually “fetal tissue.” At this age, it’s still embryonic tissue. Yes, a medical doctor speaking on behalf of tens of thousands of medical doctors made an obviously false medical statement in a sentence that was supposed to clarify medical reality. Yes, it’s the very same distinction that pro-lifers get hammered on all the time by the exact same people. (“It’s not a fetus; it’s a blastocyst!”)
No, it’s not surprising. It all makes sense once you realize that they don’t actually care about the embryo/fetus distinction; they only use these terms so they can avoid the ordinary English term: “baby.” ACOG holds pro-lifers to strictly accurate terminology for prenatal development, but they have no reason to hold themselves to the same standard.
So, the new official term is medically inaccurate. But ACOG hath spoken, and We the People are supposed to pretend that ACOG is an objective body of experts acting on pure rationality. “Fetal heartbeat” is now going to be safely suppressed for being, they say, “medically inaccurate.”
Please remember that they are lying.
I try to reserve that strong term, “lying,” for clear cases of deliberate deception. But that’s exactly what we have here.
The medically accurate, scientifically correct term is “embryonic heartbeat.” This term has been in the literature for generations. It is universally accepted and unchallenged, a poster child for “scientific consensus.” Just look at a tiny fragment of the literature:
“Embryonic Heart Rate as a Prognostic Factor for Chromosomal Abnormalities” (Journal of Ultrasound Medicine, 2009; deals with embryos younger than nine weeks)
“Evaluation of normal gestational sac growth: appearance of embryonic heartbeat and embryo body movements using the transvaginal technique.“(Obstetrics and Gynecology, 1991; deals with embryos between five to twelve weeks’ gestation) (of
“Embryonic heart rate in the early first trimester: what rate is normal?” (Journal of Ultrasound Medicine, 1995; embryos are six to eight weeks’ gestation)
“Embryonic heart rate in human pregnancy.” (Journal of Ultrasound Medicine, 1991; embryos are three to seven weeks old)
“Slow embryonic heart rate in early first trimester: indicator of poor pregnancy outcome.” (Radiology, 1994; “embryonic heart rate” is determined “prior to 8 weeks gestation”)
“Predictive value of the presence of an embryonic heartbeat for live birth: Comparison of women with and without recurrent pregnancy loss.” (Fertility and Sterility, 2004; embyronic heart rate obtained “between 6 and 8 weeks of gestation)
“Predictive value of early embryonic cardiac activity for pregnancy outcome.” (American Journal of Obstetrics and Gynecology, 1991; embryos are 5 to 9 weeks’ gestation)
“A close look at early embryonic development with the high-frequency transvaginal transducer.” (American Journal of Obstetrics and Gynecology, 1988; embryos are as young as 5 weeks 6 days when “the heartbeat appeared.”)
“What’s new in first trimester ultrasound.” (Radiologic Clinics of North America, 2003; “the primitive heart begins to beat at the end of the third week after fertilization”)
“Transvaginal versus transabdominal Doppler auscultation of fetal heart activity: A comparative study.” (American Journal of Obstetrics and Gynecology, 1996; embryos are between 6 and 9 weeks of gestation when “fetal heart rate” is detected.)
I pulled all those off Google Scholar in twenty minutes. There’s tons of them. I had room to be choosy for this article, but give me an hour and I can find a hundred more examples of peer-reviewed medical doctors and scientists talking about “embryonic heartbeat” like it’s the most natural thing in the world.
That alone doesn’t prove anything. Maybe ACOG’s official new terminology is even more popular than “embryonic heartbeat.” So now we ask: how often does the phrase “electrically induced flickering of a portion of the fetal tissue that will become the heart” show up in peer-reviewed scientific literature?
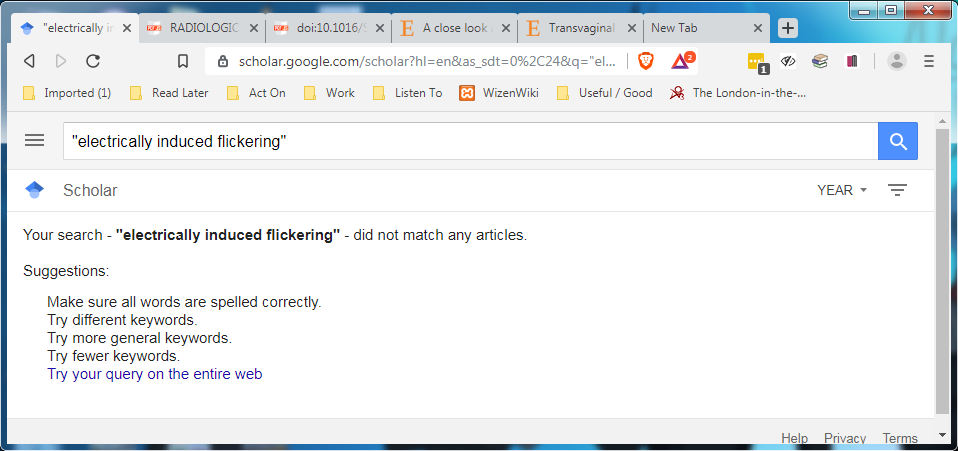
Of course, Google Scholar’s not the be-all end-all of academia, but it seems safe to say that, when Google Scholar can immediately find hundreds of matches for Phrase A, and zero matches for Phrase B, then Phrase A is the more common and scientifically accurate one.
How about the New York Times‘ even more made-up phrase, “embryonic pulsing”? That gets three matches on Google Scholar, but one’s an English paper and two are about a scanning technique. None are about embyronic heartbeats. Why? Because doctors refer to those as “embryonic heartbeats.” It’s the New York Times and its friends at The Daily Beast et. al. that doesn’t want to make the heartbeats go away. (They should re-read Poe’s “The Telltale Heart;” it will resonate!)
One more: in December 2015, Dr. Jen Gunter, a late-term abortionist who is sometimes treated as a neutral source by mainstream media, asserted that the most correct term would be “fetal pole cardiac activity.” She’s since been quoted favorably on this in outlets like Wired and Forbes. Does her euphemism have any more traction than the others? At first glance, you might think so! There are 38 results for “fetal pole cardiac activity” on Google Scholar! Doesn’t hold a candle to the 735 for “embyronic heartbeat,” but still, that shows some scientific uptake of her terminology, right?
But that’s when you realize that the matches for “fetal pole cardiac activity” are actually for lists: things like “…fetal pole, cardiac activity, and gestational sac,” or, “If a fetal pole/cardiac activity is detected…” or, “presence of a fetal pole +/- cardiac activity.” Some of the authors of these articles even appeared on my list above as users of “embryonic heartbeat!” So it appears that nobody in the literature has used the actual phrase to describe an actual embryonic heartbeat except Dr. Jen Gunter… and, of course, a mainstream media that is desperate to escape the simple, uncomfortable reality of “heartbeat.”
Now that the Cathedral has denounced the term “embryonic heartbeat” as wrongthink, you can expect it to disappear within a year or two. New articles will have the phrase stripped out and replaced with the new, politically correct terminology… even if it makes the articles less clear and less accurate. The authors of the articles I’ve cited will either keep their heads down or apologize for ever having used it. (They’re probably mostly pro-choice anyway.) Anyone who does use the term now will be accused of having “an agenda.” They’ve pulled this very same language trick before: with the beginning of pregnancy (it’s at fertilization), with the word “abortionist,” with the very idea of an “unborn child.” I already see it happening with “embryonic heartbeat.”
That’s why I wanted to get this down, on the record, before it’s washed away by the overwhelming coercive power the abortion industry can bring to bear on the scientific and journalistic communities: they are lying. The only people who have ever challenged the scientific term “embryonic heartbeat” are people who find that language politically inconvenient. It’s an uncontroversial term with consistent usage and universal acceptance that dates back decades.
So, when you hear a complaint that a “heartbeat bill” uses medically inaccurate or unscientific terminology, remember:
They are lying.
They are lying.
They are lying.
*I spent about 15 minutes trying to find a good, succinct, link that would define “the Cathedral” concept for those unfamiliar with it. But the term comes from Mencius Moldbug, who did nothing succinctly, and I don’t think anybody who has tried to boil it down has succeeded. So, sorry to throw an 11,000-word article at you in an aside, but it’s a pretty good one.
**Image credits: human heart development by OpenStax College. Fetal remains by Wikipedia user “Anatomist90.” All images used under their open CC BY 3.0 licenses.
This is the 2020 sequel to Unflattering Assessments of 2016 Presidential Candidates. I realized today that I need to get these in before candidates start dropping out like flies. I admit I am not as mean this year, but only because I refuse to devote enough mental resources to learning about “Jay Hickenlooper” and “Derek Stallwell” or whatever to render a sufficiently devastating judgment upon them.

This post was written because my family was leaving the New Bohemia in downtown Saint Paul when we passed a car with a “BETO 2020” bumper sticker on it. I pointed and laughed. My wife, who wisely does not follow politics and had no idea who “Beto” was, asked why I was laughing, and I explained that Beto stopped being cool the moment he lost to Ted Cruz. Anyone with a bumper sticker for him must either not care about coolness or be hilariously out-of-touch.
So, my wife asked, reasonably: what presidential candidates have bumper stickers that cool people put on their cars?
Remember: this isn’t a list of how cool each candidate is. This is a list of how cool each candidate’s supporters are, specifically in Saint Paul, Minnesota. Plenty of uncool candidates have cool supporters and vice versa.
1. Amy Klobuchar – she wins ONLY in Minnesota, but oh boy does she win Minnesota, Nearly everyone in Minnesota, of both sexes, including Republicans, has an irrational love of Amy, to the point where I suspect witchcraft. She’s a solid-left Democrat and workplace abuser who has somehow fooled half the state’s Republican voters into thinking she’s a nice young lady and reasonable advocate for their interests. (My mother blames Amy’s dad.) So it’s not edgy-cool to have an Amy bumper sticker in downtown St. Paul. But cool people are gonna be like, “Hey, I love Amy, that guy’s cool.”
2. Pete Buttigieg – hot stuff right now, which is bizarre for me, since I’ve followed his career since he was just some jerk, long before it occurred to me he could be President. Could stay that way because gay dudes are cool (and it turns out he’s gay? I never realized), but more likely Mayor Pete is the New Beto and will soon end up with Beto down at #25.
I was surprised to see Justice Alito joining the Supreme Court majority in Iancu v. Brunetti today.

This is a trademark case. The U.S. Trademark Office rejected a trademark for the brand “FUCT” because of a law (the Lanham Act) that says trademarks should not be granted for “immoral or scandalous matter.” The guy who runs FUCT insists that it isn’t obscene, and actually you’re supposed to pronounce it by spelling it out: F-U-C-T.
The U.S. Supreme Court decided today, 6-3, that (1) hahahaha nobody believes you, dude, and (2) nevertheless, this law violates the First Amendment. Therefore, the trademark must be granted to FUCT.
Justice Alito joined that decision. But this struck me as odd. Alito is the Supreme Court’s obscenity-hater-in-chief and its champion against moral relativism. In Snyder v. Phelps, the Supreme Court ruled that Fred Phelps and the Westboro Baptist Church could not be sued for inflicting emotional distress after their obscene protest of a dead soldier’s funeral, because of the First Amendment. In that case, Alito stood alone to dissent. He would have allowed the soldier’s family to sue Phelps for a lot of money. That’s who Alito is. You might call him the Supreme Court’s moral scold. I call him that lovingly, because I tend to agree with him.
The First Amendment protects many kinds of speech, especially political speech and its constituent activities, but also religious speech, art, and the general free exchange of ideas, information, and stories. As American culture becomes more and more polarized into two separate and isolated camps, each increasingly inclined to silence the other, we need a strong First Amendment now more than ever (hence the Court’s correct decision in Citizens United*). But the Supreme Court has repeatedly held throughout its history that the First Amendment’s protections do not extend to obscenity. Obscenity is not free speech per se, in the Court’s view.
Thus, it is perfectly legal to outlaw pornography. It has been illegal throughout nearly all of the country throughout nearly all of its history. Indeed, pornography is technically still illegal in most places today (here is Minnesota’s anti-porn statute; your state likely has a similar one)… but it’s difficult to enforce, thanks to some Supreme Court precedents that make it difficult to prove that something really is porn (not art). The barrier-smashing power of the Internet, too, has made enforcement nearly impossible.
However, Justice Alito remembers that, despite barriers to enforcing anti-obscenity laws today, obscenity is still not actually protected speech. He sometimes seems to be the only member of the Supreme Court who does.
And here he is ruling in favor of a brand called FUCT?
So I looked up his concurring opinion. And it’s good! I really like the distinctions he draws. Were I a justice on the Supreme Court, I’d join it. I’m going to reprint the whole thing here. Don’t worry; it’s short.
For the reasons explained in the opinion of the Court, the provision of the Lanham Act at issue in this case violates the Free Speech Clause of the First Amendment because it discriminates on the basis of viewpoint and cannot be fixed without rewriting the statute. Viewpoint discrimination is poison to a free society. But in many countries with constitutions or legal traditions that claim to protect freedom of speech, serious viewpoint discrimination is now tolerated, and such discrimination has become increasingly prevalent in this country. At a time when free speech is under attack, it is especially important for this Court to remain firm on the principle that the First Amendment does not tolerate viewpoint discrimination. We reaffirm that principle today.
Our decision is not based on moral relativism but on the recognition that a law banning speech deemed by government officials to be “immoral” or “scandalous” can easily be exploited for illegitimate ends. Our decision does not prevent Congress from adopting a more carefully focused statute that precludes the registration of marks containing vulgar terms that play no real part in the expression of ideas. The particular mark in question in this case could be denied registration under such a statute. The term suggested by that mark is not needed to express any idea and, in fact, as commonly used today, generally signifies nothing except emotion and a severely limited vocabulary. The registration of such marks serves only to further coarsen our popular culture. But we are not legislators and cannot substitute a new statute for the one now in force.
The full slip opinion is here; Alito’s concurrence is on pages 14 and 15 of the PDF.
*I know Scalia’s concurrence isn’t the controlling opinion in Citizens United, but it’ll be a cold day in Hell when I link favorably to a Kennedy-penned opinion in a case where literally anybody else in the majority wrote on the central question of the case.
The editor wishes to disclose that he successfully, if barely, resisted the temptation, nearly universal among bloggers this morning, to make this article’s title a “FUCT” pun.
The document and my discussion are at the bottom, if you want to skip down and read the darn thing. Otherwise, I have some introductory comments on the Catholic Church and gender issues.
For some years, I have tried to determine what the Catholic Church officially believes about people who identify as transsexual. This is not as easy as you might think.
Now, Catholicism has a great deal to say about specific sexual acts. To wit, unless it is a sexual act act that is open to life, performed freely in a loving, male-female marriage, the Catholic Church is Not For It. Several pages of the Catechism are devoted to going through common sex acts and gently, politely identifying them as gravely evil and harmful to all participants. Masturbation: bad. Fornication: bad. Prostitution: bad. Adultery: bad. Contraception: bad. And so forth. A little ways above this section, there’s a discussion of the importance of distinct maleness and femaleness, their complementarity, their role in driving humans to communion with one another, and how they figure in God’s overall plan for humanity.
This, then, is where we find the Catechism’s condemnation of all homosexual acts, although the authors take pains to clarify that the Church does not condemn homosexual persons. Gay and lesbian Catholics cannot, after all, be “open to life” in sex acts with members of the same sex. Even if they could, these acts would not conform to the Church’s understanding of complementarity between the sexes. Since all Catholics, including gay and lesbian Catholics, are called to chastity, this pretty clearly rules out sexual gratification of any kind within a same-sex relationship. (The Catechism notoriously fails to suggest what positive vocations gay and lesbian Catholics might be called to, but that’s another story.)
But being transsexual is not at all the same as being gay. Some people experience an interior sensation that their apparent physical sex is incorrect. People who appear to be males (and even have male genitalia) believe themselves to be truly female, and vice versa. Often, they say they are “trapped in” or were “born into” the “wrong body.” We call these people “transsexuals.”
(To be clear: I am talking in this post specifically about transsexuals, those who desire to transform their bodies to reflect their perceived sex. There is a broader movement of “trans*” identities, which includes identification such as “bigender,” “agender,” and “genderqueer.” I confess I cannot make heads or tails of these identities, and suspect that those using them are using a definition of “gender” so subjective as to be either trivial or meaningless or both. Perhaps this subjectivity is considered a justified reaction against socially-imposed gender roles, which are real and often oppressive. In any event, this post is not about trans* identities broadly. I am aware that “transsexual” is now seen as somewhat archaic, but I am unaware of any more modern term that specifically identifies this particular subset of trans* persons)
In many ways, the transsexual experience runs directly counter to the prevailing narrative of the LGBT movement. Where gays, lesbians, and many trans* individuals insist that gender doesn’t matter at all, because “love is love” and identity is completely plastic, trans* people experience deep, profound alienation from their bodies, because they gender matters more than practically anything else. Their dysphoria is not remotely plastic, much to their regret. Our culture, led by the LGB movement at large, has worked very hard to imagine that all gender differences are the result of social conditioning and kyriarchy, a kind of gender nominalism that finds its apex in the same-sex marriage movement. But transsexual people affirm a kind of gender realism that has become almost alien to our culture–at least, outside of the Catholic Church.